
Certified Professional Coder (CPC) Exam
Last Update Jul 26, 2026
Total Questions : 453
We are offering FREE CPC AAPC exam questions. All you do is to just go and sign up. Give your details, prepare CPC free exam questions and then go for complete pool of Certified Professional Coder (CPC) Exam test questions that will help you more.


(The patient presents to the emergency department with chest pain. EKG showsNSTEMIand troponin is abnormal. The ED provider discusses the case with a cardiologist and the patient is admitted for heart catheterization/PCI. What is the E/M service and ICD-10-CM coding reported for the ED provider?)
A suppression study includes five glucose tests and five growth hormone tests.
What CPT® coding is reported?
(A 58-year-old patient undergoes diagnostic facet joint injections. The physician performsbilateral paravertebral facet joint injectionsat theT2–T3, T3–T4, and T4–T5levels, usingfluoroscopic guidanceat each site. What CPT® coding is reported for this encounter?)
(A dermatologist excises abasal celllesion from an area of thescalp, measuring3.7 cm. This is closed with alayered repair. What CPT® and ICD-10-CM codes are reported?)
(ESTABLISHED PATIENT VISIT: A 37-year-old woman presents with coughing, congestion, upper respiratory symptoms, and headache for two days. Complete ROS negative except as noted. No significant past/family history. Exam: stable vitals, nasal congestion, normal TMs, occasional rhonchi, no wheezing, normal heart, soft abdomen. Assessment/Plan:Acute upper respiratory infection, fluids,amoxicillinfor 5–7 days, return precautions. What CPT® code is reported?)
A patient with end-stage renal disease (ESRD) receives hemodialysis 3x weekly in the office for one month. The nephrologist performs a comprehensive exam and supervises dialysis.
What CPT® and ICD-10-CM codes are reported?
A patient who has colon adenocarcinoma undergoes an open partial colectomy. The surgeon removes the proximal colon and terminal ileum and reconnects the cut ends of the distal ileum and
remaining colon.
What procedure and diagnosis codes are reported?
A 78-year-old patient experiencing intermittent asthma with exacerbation is in her pulmonologist ' s office for a pulmonary function test. The pulmonologist tests for spirometry, vital capacity,
breathing capacity, and flow volume capturing the measurements before and after administering a bronchodilator.
What CPT® and ICD-10-CM codes are reported?
A 45-year-old patient comes In with chronic sinusitis that has not responded to medication. The physician decides to use a sinus stent implant to help alleviate the patients symptoms.
The physician inserts the implant into the ethmoid sinus using a delivery system. This implant is designed to keep the surgical opening clear, prop open the sinus, and gradually release a corticosteroid with anti-inflammatory properties directly to the sinus lining. The implant is not permanent and will dissolve over time.
What HCPCS Level II code is reported?
The gastroenterologist performs a simple excision of three external hemorrhoids and one internal hemorrhoid, each lying along the left lateral column. The operative report indicates that the internal hemorrhoid is not prolapsed and is outside of the anal canal.
What CPT® and ICD-10CM codes are reported?
Ms. C is diagnosed with a supratentorial intracerebral hematoma, and the neurologist performs a craniectomy to access the hematoma. The hematoma is accessed, and a suction device is
used to remove it.
What CPT@ code is reported?
A patient undergoes a percutaneous liver biopsy with ultrasound guidance for primary biliary cirrhosis.
What CPT® and ICD-10-CM codes are reported?
A patient that delivered her second child vaginally has a history of having a previous cesarean delivery for the first child.
What CPT® code is reported for the delivery of the second child with antepartum care and postpartum care with the same provider?
A 3-day-old died in her sleep. The pediatrician determined this was the result of crib death syndrome. The parents give permission to refer the newborn for a necropsy. The pathologist receives the newborn with her brain and performs a gross and microscopic examination. The physician issues the findings and reports they are consistent with a normal female newborn.
What CPT® code is reported?
A pediatric patient with a congenital double inlet ventricle undergoes corrective cardiac surgery. The surgeon performs a modified Fontan procedure to redirect systemic venous blood flow directly to the pulmonary arteries as part of staged repair for a single-ventricle physiology.
What CPT® and ICD-10-CM® codes are reported?
A wedge excision of soft tissue at the lateral margin of an ingrown toenail on the left great toe is performed.
What CPT® code is reported?
Refer to the supplemental information when answering this question:
View MR 903096
What CPT® and ICD-10-CM coding is reported?
Which HCPCS Level II codes identify temporary services that would not be assigned a CPT® code, but are needed for claims processing purposes?
A 64-year-old with congestive heart failure (CHF) has pericardial effusion. The provider inserts a needle under ultrasound guidance, aspirating the fluid from the pericardial sac.
What CPT® coding is reported?
Refer to the supplemental information when answering this question:
View MR 004813
What CPT® and ICD-10-CM codes are reported?
A 55-year-old patient was recently diagnosed with an enlarged goiter. It has been two years since her last visit to the endocrinologist. A new doctor in the exact same specialty group will be examining her. The physician performs a medically appropriate history and exam. The provider reviewed the TSH results and ultrasound. The provider orders a fine needle aspiration biopsy which is a minor procedure.
What E/M code is reported?
Which place of service code is submitted on the claim for a service that is performed in a skilled nursing facility?
A patient ' s left eye is damaged beyond repair due to a work injury. The provider fabricates a prosthesis from silicon materials and makes modifications to restore the patient ' s cosmetic appearance.
What CPT® code is reported?
A CRNA independently administers MAC anesthesia for ICD replacement.
What CPT® and ICD-10-CM codes are reported?
(A 42-year-old female is in the operative room to repair azone 2 flexor digitorum profundus (FDP) tendonlaceration involving her index finger with an associatedradial digital nerveinjury. The dorsal side of the FDP tendon was sutured. Next, themicroscopewas brought into place and the radial digital nerve was repaired using epineural sutures. What CPT® codes are reported?)
Preoperative diagnosis: Right thigh benign congenital hairy nevus. *1
Postoperative diagnosis: Right thigh benign congenital hairy 0 nevus.
Operation performed: Excision of right thigh benign congenital > 1
nevus, excision size with margins 4.5 cm and closure size 5 cm.
Anesthesia: General.0
Intraoperative antibiotics: Ancef.0
Indications: The patient is a 5-year-old girl who presented with her parents for evaluation of her right thigh congenital nevus. It has been followed by pediatrics and thought to have changed over the past year. Family requested excision. They understood the risks involved, which included but were not limited to risks of general
anesthesia, infection, bleeding, wound dehiscence, and poor scar formation. They understood the scar would likely widen as the child grows because of the location of it and because of the age of the patient. They consented to proceed.
Description of procedure: The patient was seen preoperatively in > I the holding area, identified, and then brought to the operating room. Once adequate general anesthesia had been induced, the patient ' s right thigh was prepped and draped in standard surgical fashion. An elliptical excision measuring 6 x 1.8 cm had been marked. This was injected with Lidocaine with epinephrine, total of 6 cc of 1% with 1:100,000. After an adequate amount of time, a #15 blade was used to sharply excise this full thickness.
This was passed to pathology for review. The wound required □ limited undermining in the deep subcutaneous plane on both sides for approximately 1.5 cm in order to allow mobilization of the skin for closure. The skin was then closed in a layered fashion using 3-0 Vicryl on the dermis and then 4-0 Monocryl running subcuticular in the skin, the wound was cleaned and dressed with Dermabond and Steri-Strips.
The patient was then cleaned and turned over to anesthesia for S extubation.
She was extubated successfully in the operating room and taken S to the recovery room in stable condition. There were no complications.
What CPT® codes are reported?
A patient has squamous cell carcinoma lesions destroyed with cryosurgery:
0.6 cm right dorsal foot
2.0 cm left dorsal foot
What CPT® coding is reported?
According to the ICD-10-CM coding guidelines, when coding hypertension with heart conditions classified to I50.- or I51.4–I51.7, I51.89, I51.9, what category should be used?
A 13-year-old established patient is seen for an annual preventive exam. Last visit was two years ago.
What CPT® code is reported?
A patient arrived at the emergency department experiencing pain in both legs. The ED physician ordered a comprehensive duplex scan of the arteries in both lower extremities to rule out arteriosclerosis.
What CPT® and ICD-10-CM codes are reported?
A 6-French sheath and catheter is placed into the coronary artery and is advanced to the left side of the heart into the ventricle. Ventriculography is performed using power injection of contrast agent. Pressures in the left heart are obtained. The coronary arteries are also selected and imaged.
What CPT® code is reported?
A 57-year-old woman with a physical status of 3 received general endotracheal anesthesia for a panniculectomy. The anesthesiologist personally performed the entire anesthesia service.
What CPT@ coding is reported for the anesthesia?
A physician sees a patient for the first observation visit, spends 85 minutes, with moderate MDM.
What CPT® code is reported?
A patient is brought to the operating room with a right-sided peripheral vertigo. The provider makes a postauricular incision and uses an operating microscope to perform a mastoidectomy using a burr. He next destroys the semicircular canals, the utricle, and saccule completely removing the diseased labyrinth structures. The provider sutures the incision.
What CPT® code and ICD-10-CM codes are reported?
A patient presents with fever, cough, SOB, and fatigue. PCR test is positive for COVID-19. Final diagnosis: pneumonia due to COVID-19. What ICD-10-CM coding is reported?
(A wheelchair-bound resident of a skilled nursing facility is seen in the physician’s office. The physician’s office makes arrangements with a social worker to take the patient back to the skilled nursing facility. What is the HCPCS Level II transportation service code?)
A patient is diagnosed with diabetic polyneuropathy.
Using ICD-10-CM coding guidelines, what ICD-10-CM coding is reported?
A 32-year-old vialled a provider due to skin itching and ongoing irritation and watering of the eyes. Suspecting an allergy, the provider suspects an allergic reaction and decides to conduct allergy testing. A prick on the skin of the patient ' s forearm is performed by introducing a small amount of an allergen and monitored for signs of an allergic reaction.
What CPT® code is reported?
(A patient with age-related osteoporosis is hospitalized after a slip and fall resulting in fractures to both hips. The physician ordersthree-view imaging of both hips and the pelvis, interpreted by the hospital radiologist. Later the same day, the patient falls from bed and the doctor ordersthree additional viewsof both hips and pelvis, interpreted by thesame radiologist. What CPT® coding is reported?)
A patient returns for embryo transfer. The lab thaws cryopreserved embryos and cultures them for two additional days.
What CPT® coding is reported?
View MR 001394
MR 001394
Operative Report
Procedure: Excision of 11 cm back lesion with rotation flap repair.
Preoperative Diagnosis: Basal cell carcinoma
Postoperative Diagnosis: Same
Anesthesia: 1% Xylocaine solution with epinephrine warmed and buffered and injected slowly through a 30-gauge needle for the patient ' s comfort.
Location: Back
Size of Excision: 11 cm
Estimated Blood Loss: Minimal
Complications: None
Specimen: Sent to the lab in saline for frozen section margin control.
Procedure: The patient was taken to our surgical suite, placed in a comfortable position, prepped and draped, and locally anesthetized in the usual sterile fashion. A #15 scalpel blade was used to excise the basal cell carcinoma plus a margin of normal skin in a circular fashion in the natural relaxed skin tension lines as much as possible The lesion was removed full thickness including epidermis, dermis, and partial thickness subcutaneous tissues. The wound was then spot electro desiccated for hemorrhage control. The specimen was sent to the lab on saline for frozen section.
Rotation flap repair of defect created by foil thickness frozen section excision of basal cell carcinoma of the back. We were able to devise a 12 sq cm flap and advance it using rotation flap closure technique. This will prevent infection, dehiscence, and help reconstruct the area to approximate the situation as it was prior to surgical excision diminishing the risk of significant pain and distortion of the anatomy in the area. This was advanced medially to close the defect with 5 0 Vicryl and 6-0 Prolene stitches.
What CPT® coding is reported for this case?
(A patient is seen for nausea, vomiting, and sharp right lower abdominal pain. CT and labs support a diagnosis ofchronic appendicitis. The physician schedules anopen appendectomyand removes the appendix. What CPT® and diagnosis codes are reported?)
When a provider ' s documentation refers to use, abuse, and dependence of the same substance (e.g. alcohol), which statement is correct?
(Full Case:Preoperative diagnosis:Recurrent dysphagia.Postoperative diagnosis:Hiatal hernia with obstruction.Procedure:EGD with dilation.Consent:PAR conference; informed consent signed; premedication given.Position/monitoring:left lateral decubitus; monitored with BP cuff and pulse oximeter throughout.Topical:Hurricaine spray to posterior pharynx.Scope passage:flexible endoscope passed under direct visualization through cricopharyngeus into esophagus; advanced with identification of EG junction into stomach; rugal folds visualized; advanced to antrum/pylorus; pylorus cannulated; duodenal bulb and second portion visualized; retroflexed views of cardia/fundus/lesser curvature.Dilation technique:guidewire placed in antrum; scope removed; wire positioned by markings;#14 French dilatorpassed into stomach area;esophageal dilation performed over guidewire.Findings:tortuous/shortened esophagus; large sliding hiatal hernia; EG junction ~30 cm; stomach abnormal with very large sliding hiatal hernia; duodenum normal.Question:What CPT® coding is reported?)
A patient presents with 26 skin tags on the neck and shoulder. The provider removes all using a scissoring technique.
What CPT® coding is reported?
What modifier is appended to indicate when a service is performed because it was mandated by a third-party payer, government agency, or other regulatory requirement?
(Which punctuation is used in the ICD-10-CM Tabular List to denotesynonyms, alternative wording, or explanatory phrases?)
Refer to the supplemental information when answering this question:
View MR 138093
What E/M coding is reported?
Refer to the supplemental information when answering this question:
View MR 874276
What E/M code is reported?
Refer to the supplemental information when answering this question:
View MR 354859
What CPT® and ICD-10-CM coding is reported?
A patient with suspected gynecologic malignancy undergoes laparoscopic staging including bilateral pelvic lymphadenectomy, periaortic lymph node sampling, peritoneal washings, peritoneal and diaphragmatic biopsies, and omentectomy.
What CPT® coding is reported?
A 32-year-old is in the outpatient clinic for an esophagoscopy due to increased difficulty swallowing with his eosinophilic esophagitis. The flexible scope is inserted in the mouth and into the
esophagus. Examination of the esophagus noted narrowing in the distal esophagus. Following an injection of Kenalog, a transendoscopic balloon dilation was performed in the area of
stenosis. Inflation was repeated eventually reaching 18 mm in diameter. What CPT® coding is reported for this procedure?
The CPT® code book provides full descriptions of medical procedures, although some descriptions require the use of a semicolon (;) to distinguish among closely related procedures.
What is the full description of CPT® code 44361?
Refer to the supplemental information when answering this question:
View MR 005271
What CPT® coding is reported?
A 45-year-old patient presents with right shoulder pain. The provider administers three trigger point injections in the trapezius muscle and two in the pectoralis muscle.
What CPT® coding is reported?
An interventional radiologist performs an abdominal paracentesis in his office utilizing ultrasonic imaging guidance to remove excess fluid. What CPT® coding is reported?
An inpatient, suffering from hypertension and chronic kidney disease, is administered continuous venovenous hemofiltration. The on-duty nephrologist performs a series repeated low-level evaluation and management services to monitor the patient ' s status.
What is the CPT® and ICD-10-CM coding '
A patient is diagnosed with sepsis and associated acute respiratory failure.
What ICD-10-CM code selection is reported?
(An orthopedic surgeon evaluated a patient in the emergency room two months after a surgical repair of a right radius and ulnar shaft fracture. After reinjury, imaging shows a displaced proximal fixation screw andmalunion of only the radial shaft. The same surgeon performs surgery to repair the malunion using a graft from the hip. What CPT® and diagnosis codes are reported?)
(A patient presents with dysuria and lower abdominal pain. The physician suspects UTI. Anautomated urinalysis without microscopyis done in the office and isnegative. UTI is ruled out for the final diagnosis. What CPT® and ICD-10-CM codes are reported?)
The gynecologist performs a colposcopy of the cervix including biopsy and endocervical curettage.
What CPT® code is reported?
A Medicare patient that is on dialysis for ESRD is seen by the nurse for a Hep B vaccination. This patient is given a dialysis patient dosage as part of a three-dose schedule. The nurse administers the Hep B vaccine in the right deltoid. The physician reviews the chart and signs off on the nurse ' s note.
What procedure and diagnosis codes are reported for the scheduled vaccine injection for this Medicare patient?
Patient has undergone open surgery for a left total knee arthroplasty. While in the recovery room, he continued to have severe postoperative pain. The surgeon ordered a femoral block for postoperative pain. The anesthesiologist evaluated the patient and performed a left femoral block, which provided significant post-operative pain relief.
What CPT® coding is reported?
View MR 099405
MR 099405
CC: Shortness of breath
HPI: 16-year-old female comes into the ED for shortness of breath for the last two days. She is an asthmatic.
Current medications being used to treat symptoms is Advair, which is not working and breathing is getting worse. Does not feel that Advair has been helping. Patient tried Albuterol for persistent coughing, is not helping. Coughing 10-15 minutes at a time. Patient has used the Albuterol 3x in the last 16 hrs. ED physician admits her to observation status.
ROS: No fever, no headache. No purulent discharge from the eyes. No earache. No nasal discharge or sore throat. No swollen glands in the neck. No palpitations. Dyspnea and cough. Some chest pain. No nausea or vomiting. No abdominal pain, diarrhea, or constipation.
PMH: Asthma
SH: Lives with both parents.
FH: Family hx of asthma, paternal side
ALLERGIES: PCN-200 CAPS. Allergies have been reviewed with child’s family and no changes reported.
PE: General appearance: normal, alert. Talks in sentences. Pink lips and cheeks. Oriented. Well developed. Well nourished. Well hydrated.
Eyes: normal. External eye: no hyperemia of the conjunctiva. No discharge from the conjunctiva
Ears: general/bilateral. TM: normal. Nose: rhinorrhea. Pharynx/Oropharynx: normal. Neck: normal.
Lymph nodes: normal.
Lungs: before Albuterol neb, mode air entry b/l. No rales, rhonchi or wheezes. After Albuterol neb. improvement of air entry b/l. Respiratory movements were normal. No intercostals inspiratory retraction was observed.
Cardiovascular system: normal. Heart rate and rhythm normal. Heart sounds normal. No murmurs were heard.
GI: abdomen normal with no tenderness or masses. Normal bowel sounds. No hepatosplenomegaly
Skin: normal warm and dry. Pink well perfused
Musculoskeletal system patient indicates lower to mid back pain when she lies down on her back and when she rolls over. No CVA tenderness.
Assessment: Asthma, acute exacerbation
Plan: Will keep her in observation overnight. Will administer oral steroids and breathing treatment. CXR ordered and to be taken in the morning.
What E/M code is reported?
A 30-year-old patient with a scalp defect is having plastic surgery to insert tissue expanders. The provider inserts the implants, closes the skin, and increases the volume of the expanders by injecting saline solution. Tissue is expanded until a satisfactory aesthetic outcome is obtained to repair the scalp defect.
What CPT® code is reported?
A patient presents with fever, cough, SOB, and a recent history of COVID-19. A PCR test was positive for COVID-19. The provider documents a final diagnosis of “pneumonia with history of COVID-19.”
What ICD-10-CM coding is reported?
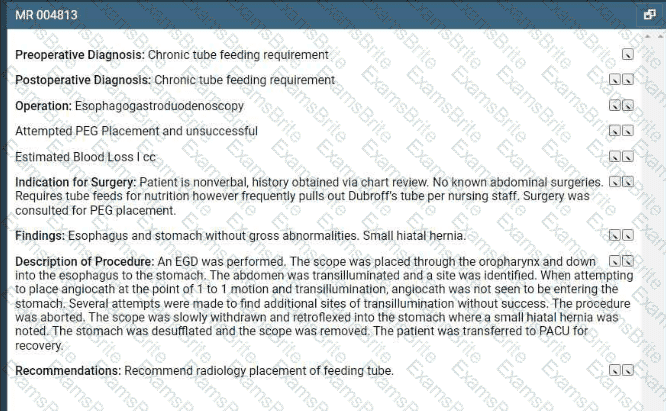
A patient arrives for a PEG placement. The patient requires tube feeds for nutrition but frequently pulls out the dobhoffs tube. An EGD was performed. Several attempts were made to place the
PEG tube without success so the procedure was aborted. During the withdraw of the scope, a small hiatal hernia was noted in the stomach. The scope was removed the the patient transferred
to recovery.
What CPT and ICD-10-CM coding is reported?
A business requires drug testing for cocaine and methamphetamines prior to hiring a job candidate. A single analysis with direct optical observation is performed, followed by a confirmation for cocaine.
Which codes are used for reporting the testing and confirmation?
(A patient has aliver massand presents for apercutaneous needle biopsy of the liver with CT guidance. Four core specimens are taken to rule out benign hepatic adenoma. What CPT® and ICD-10-CM codes are reported?)
A 62-year-old with ventricular fibrillation comes to the outpatient surgery department for the replacement of a pacing cardioverter-defibrillator. The procedure is performed under MAC
anesthesia. The Certified Registered Nurse Anesthetist (CRNA), is working independently without medical direction.
What CPT® and ICD-10-CM codes are reported for the CRNA?
A patient is diagnosed with sepsis due to enterococcus. What ICD-10-CM code is reported?
When a provider’s documentation refers to use, abuse, and dependence of the same substance (e.g., alcohol), which statement is correct?
A patient presents to the emergency room with a nosebleed that is controlled by limited anterior nasal packing.
What CPT® code is reported?
(A patient is in the operating room for a planned partial meniscectomy of the temporomandibular joint. However, after general anesthesia was administered and the oral surgeon made the incision, the patient experienced respiratory distress. The oral surgeon decides tocancel the procedure. What CPT® coding is reported for the oral surgeon?)
A surgeon performs a complete bilateral mastectomy with insertion of breast prosthesis at the same surgical session.
What CPT@ coding is reported?
(A patient is seen by her podiatrist to treat a painfulleft ingrown toenailon the big toe. The podiatrist performs awedge excisionof the skin of the nail fold at the lateral margin. Local anesthetic is administered, and an elliptical incision is made through subcutaneous tissue of the affected nail groove. A wedge-shaped piece of soft tissue from the nail margins is removed. What CPT® code is reported?)
A patient receives 200 mg IM Depo-Testosterone.
What HCPCS Level II coding is reported?
(Full Case:Patient:V. Bowen.Physician:C.S., MD.Reason for admission:Abdominal pain.HPI:admitted this morning; sudden onset RUQ pain began ~4:00 p.m. yesterday; started while eating; 8/10; chills/sweating/nausea; no vomiting/diarrhea; last BM 2:00 p.m. yesterday; unable to pass stool or gas since; abdominal distention; poor sleep; prior similar episodes relieved by gas tablets but not this time; no discolored stool/urine.PMH:HTN (losartan; missed dose).PSH:bunion surgery right foot.FH:HTN.SH:no smoking/alcohol.Meds:losartan daily.Allergies:NKDA.ROS:nausea, no emesis; no flatus/stool since yesterday; no weight change; no SOB/chest pain; no jaundice; no urinary frequency/urgency.PE:alert/oriented x3; obvious abdominal discomfort. Vitals 139/100, pulse 100, RR 16, temp 36.4. HEENT normal; CV regular; lungs clear. Abdomen: +BS, soft but very tender; worst RUQ;Murphy’s sign; guarding and rebound (worse with palpation). Extremities trace edema.Labs ordered/reviewed:CMP with abnormal LFT/bili; CBC WBC 9.9; etc.Final assessment:RUQ abdominal pain,rule out cholecystitis.Plan:NPO; morphine IV (controlled substance); IV NS 150 cc/hr; abdominal ultrasound and HIDA ordered; consider surgical consult based on results.Question:What CPT® and ICD-10-CM codes are reported?)
What ICD-10-CM coding is reported for a patient who has hypertension and CKD stage 2?
(A patient presents for surgery due to recurrent lumbar radiculopathy at a previously operated spinal level. The surgeon performs arepeat exploration laminotomywithbilateral foraminotomyto decompress nerve roots at theL1–L2 interspace. No additional spinal levels are treated. What CPT® coding is reported?)
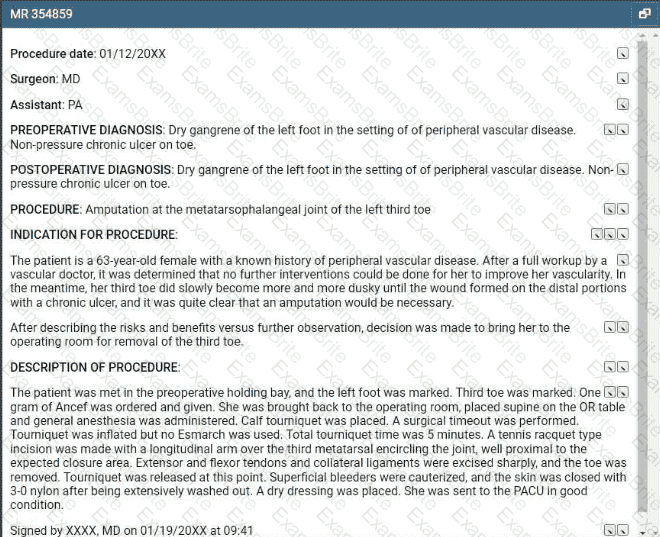
(Procedure date:01/12/20XX
Surgeon:MD |Assistant:PA
Preoperative diagnosis:Dry gangrene of the left foot in the setting of peripheral vascular disease. Non-pressure chronic ulcer on toe.
Postoperative diagnosis:Dry gangrene of the left foot in the setting of peripheral vascular disease. Non-pressure chronic ulcer on toe.
Procedure:Amputation at the metatarsophalangeal joint of the left third toe
Indication:63-year-old female with peripheral vascular disease; vascular workup determined no further interventions to improve vascularity; third toe became progressively dusky; wound formed distally with chronic ulcer; amputation necessary; risks/benefits discussed.
Description:Left foot and third toe marked; 1 g Ancef given; general anesthesia; supine; calf tourniquet; timeout; tourniquet inflated (no Esmarch); total tourniquet time 5 minutes; tennis racquet incision with longitudinal arm over third metatarsal encircling joint proximal to closure; extensor/flexor tendons and collateral ligaments excised sharply; toe removed; tourniquet released; superficial bleeders cauterized; washed out; skin closed with 3-0 nylon; dry dressing; to PACU in good condition; signed 01/19/20XX 09:41.
Question:What CPT® and ICD-10-CM coding is reported?)
Regarding the CPT® Surgery Guidelines for a surgical code designated as a " Separate Procedure " , which statement is FALSE?
A provider performs a mastoidectomy and complete labyrinthectomy for right-sided peripheral vertigo.
What CPT® and ICD-10-CM codes are reported?
(A three-year-old patient returns forstage 2treatment for double right outlet syndrome. The surgeon removes apulmonary artery bandand performstransposition repair of the great vesselsvia aortic pulmonary reconstruction. Central cannulae are inserted forECMO bypass, chemical cardioplegia is initiated, and a physician assistant monitors vitals and oxygenation until heart function resumes. What CPT® codes are reported for the surgery today?)
In medical terminology, suffixes indicate the procedure, condition, disorder, or disease.
Which term contains a suffix?
Which punctuation is used in the ICD-10-CM Alphabetic Index to identify manifestation codes?
A surgeon performed Mohs micrographic surgery on a lesion on the right arm. This required one stage with six tissue blocks.
What CPT@ codes are reported for the Mohs surgery?
A 46-year-old female is admitted to the hospital by her urologist for a left ureteral calculus. The urologist visits her again on day two and performs a low for number and complexity of problems
addressed, minimal for amount and/or complexity of data to be reviewed and analyzed, and moderate for risk of complications.
What E/M service is reported for day two?
A catheter is placed from the femoral artery into the right common carotid, with imaging of the ipsilateral extracranial carotid and bilateral external carotids.
Which CPT® codes are reported?
A patient is diagnosed with compression fractures of the C6, C7 and T1 vertebrae. The patient agrees to have vertebroplasty. Bone cement is injected in the vertebral space until each of the two whole vertebral body is filled. The procedure is performed bilaterally.
What CPT® coding is reported?
A patient has five biopsies performed on the duodenum.
What CPT® coding is reported?
(Chief Complaint: Palpable lump in the left breast. Adiagnostic mammogram (unilateral)was performed on theleft breastusingdigital imaging with CAD, with standard and additional views. What CPT® codes are reported for the radiological services?)
A 47-year-old male recently injured as a passenger in a car accident sustained multiple fractures. The patient now has physical restraints due to pulling out foley catheter, IV catheters and
attempted to pull out NG tube. Emergency department physician is asked to come see patient and injects 0.5 lidocaine into lumbar region of the spine. An indwelling catheter is placed into the
lumbar region for continuous infusion with fluoroscopy for pain management.
What CPT® is reported for the Emergency department physician?
The procedure is performed at an outpatient radiology department. From a left femoral access, the catheter is placed in the abdominal aorta and is then selectively placed in the celiac trunk and manipulated up into the common hepatic artery for an abdominal angiography. Dye is injected, and imaging is obtained. The provider performs the supervision and interpretation.
What CPT® codes are reported?
An 8-year-old undergoes tonsillectomy with adenoidectomy for chronic tonsillitis and adenoiditis with hypertrophy.
What CPT® and ICD-10-CM codes are reported?
(A 3-year-old is seen by his primary care physician for anannual exam. His last exam with the primary care physician wastwo years ago. He has no complaints. What CPT® code is reported?)
A 1-year-old patient has bilateral supernumerary digits:
Left digit contains bone and joint → amputated
Right digit is a soft-tissue nubbin → simple excision
What CPT® coding is reported?
A 50-year-old patient presented with a persistent cough has not responded to standard treatments. The patient ' s physician decides to perform a flexible bronchoscopy with bronchial biopsies to further investigate the cause. A flexible bronchoscope is inserted through the patient ' s mouth and into the bronchial tubes. Five biopsies are taken for further testing. The biopsies were sent to the lab for analysis to determine the next steps in the patient ' s treatment plan.
What CPT® coding is reported?
A surgeon performs midface LeFort I reconstruction on a patient’s facial bones to correct a congenital deformity. The reconstruction is performed in two pieces in moving the upper jawbone forward and repositioning the teeth of the maxilla of the mid face.
What CPT® code is reported?
Which is a TRUE statement for Place of Service (POS) codes for professional claims?
A patient presents with recurrent spontaneous episodes of dizziness of unclear etiology. Caloric vestibular testing is performed irrigating both ears with warm and cold water while evaluating the patient’s eye movements. There is a total of three irrigations.
What CPT® coding is reported?
A 26-year-old male presents with a deep laceration from a kitchen knife to his right hand. The surgeon washes the open wound with sterile saline. Clamps are applied. The provider cleans the
vessel and prepares the edges of thee wound. She then repairs the bleeding vessel with sutures. The clamps are removed and the provider uses a Doppler probe to check the blood flow pattern
through the repaired vessel.
What CPT® code is reported?
A patient has swelling in both arms and lymphangitis is suspected. She is in the outpatient radiology department for a lymphangiography of both arms.
What CPT® coding is correct?
A 5-year-old who has an allergy history experienced a possible reaction to peanuts. A quantitative, high-sensitive fluorescent enzyme immunoassay was used to measure specific IgE for recombinant peanut components. Results showed there was no reaction indicating the child has a peanut allergy.
What lab test is reported?
Preoperative diagnosis: Right thigh benign congenital hairy nevus. *1
Postoperative diagnosis: Right thigh benign congenital hairy 0 nevus.
Operation performed: Excision of right thigh benign congenital > 1
nevus, excision size with margins 4.5 cm and closure size 5 cm.
Anesthesia: General.0
Intraoperative antibiotics: Ancef.0
Indications: The patient is a 5-year-old girl who presented with her parents for evaluation of her right thigh congenital nevus. It has been followed by pediatrics and thought to have changed over the past year. Family requested excision. They understood the risks involved, which included but were not limited to risks of general
anesthesia, infection, bleeding, wound dehiscence, and poor scar formation. They understood the scar would likely widen as the child grows because of the location of it and because of the age of the patient. They consented to proceed.
Description of procedure: The patient was seen preoperatively in > I the holding area, identified, and then brought to the operating room. Once adequate general anesthesia had been induced, the patient ' s right thigh was prepped and draped in standard surgical fashion. An elliptical excision measuring 6 x 1.8 cm had been marked. This was injected with Lidocaine with epinephrine, total of 6 cc of 1% with 1:100,000. After an adequate amount of time, a #15 blade was used to sharply excise this full thickness.
This was passed to pathology for review. The wound required □ limited undermining in the deep subcutaneous plane on both sides for approximately 1.5 cm in order to allow mobilization of the skin for closure. The skin was then closed in a layered fashion using 3-0 Vicryl on the dermis and then 4-0 Monocryl running subcuticular in the skin, the wound was cleaned and dressed with Dermabond and Steri-Strips.
The patient was then cleaned and turned over to anesthesia for S extubation.
She was extubated successfully in the operating room and taken S to the recovery room in stable condition. There were no complications.
What CPT® coding is reported?
A 7-year-old boy is brought to the pediatric clinic by his mother. She reported that her son is complaining of discomfort in both ears and loss of hearing in the left ear for the past two days. The pediatrician diagnosis is impacted cerumen. Pediatrician with the mother ' s consent removes impacted cerumen using water irrigation In the right ear. For the left ear the cerumen impaction is removed using instrumentation.
What CPT® coding is reported '
A patient is going to have placement of a myringotomy tube. This tube is placed in the ______ to drain excess fluid.
A patient has a 5 cm tumor in the left lower quadrant abdominal wall, excised through dermis and subcutaneous tissue. Pathology is pending to rule out cancer.
What CPT® and ICD-10-CM codes are reported?
Preoperative diagnosis: Right thigh benign congenital hairy nevus. *1
Postoperative diagnosis: Right thigh benign congenital hairy 0 nevus.
Operation performed: Excision of right thigh benign congenital > 1
nevus, excision size with margins 4.5 cm and closure size 5 cm.
Anesthesia: General.0
Intraoperative antibiotics: Ancef.0
Indications: The patient is a 5-year-old girl who presented with her parents for evaluation of her right thigh congenital nevus. It has been followed by pediatrics and thought to have changed over the past year. Family requested excision. They understood the risks involved, which included but were not limited to risks of general
anesthesia, infection, bleeding, wound dehiscence, and poor scar formation. They understood the scar would likely widen as the child grows because of the location of it and because of the age of the patient. They consented to proceed.
Description of procedure: The patient was seen preoperatively in > I the holding area, identified, and then brought to the operating room. Once adequate general anesthesia had been induced, the patient ' s right thigh was prepped and draped in standard surgical fashion. An elliptical excision measuring 6 x 1.8 cm had been marked. This was injected with Lidocaine with epinephrine, total of 6 cc of 1% with 1:100,000. After an adequate amount of time, a #15 blade was used to sharply excise this full thickness.
This was passed to pathology for review. The wound required □ limited undermining in the deep subcutaneous plane on both sides for approximately 1.5 cm in order to allow mobilization of the skin for closure. The skin was then closed in a layered fashion using 3-0 Vicryl on the dermis and then 4-0 Monocryl running subcuticular in the skin, the wound was cleaned and dressed with Dermabond and Steri-Strips.
The patient was then cleaned and turned over to anesthesia for S extubation.
She was extubated successfully in the operating room and taken S to the recovery room in stable condition. There were no complications.
Which CPT® and ICD-10-CM codes are reported for this procedure?
A 45-year-old has a dislocated patella in the left knee after a car accident. She taken to the hospital by EMS for surgical treatment. In the surgery suite, the patient is placed under general anesthesia. After being prepped and draped, the surgeon makes an incision above the knee joint in front of the patella. Dissection is carried through soft tissue and reaching the patella in attempt to reduce the dislocation. When the patella is exposed, it is severely damaged due to cartilage breakdown. The tendon is dissected and using a saw the entire patella is freed and removed. The tendon sheath is closed with sutures.
What procedure code is reported for this surgery?
(Preoperative diagnoses:Bradycardia.
Postoperative diagnosis:Bradycardia.
Procedure performed:Dual-chamber pacemaker implantation.
Brief history:77-year-old female with recurrent syncope; evaluation revealed first-degree AV block, sinus bradycardia, bundle-branch block; bradyarrhythmia suspected; after discussion with her sister, dual-chamber pacemaker recommended; risks explained; consent obtained.
Procedure details:Taken to cardiac catheterization lab; positioned on cath table; prepped/draped standard; procedure challenging due to agitation despite adequate sedation; left infraclavicular area anesthetized with 0.5 cc Xylocaine; pacemaker pocket created; hemostasis with cautery; 9-French peel-away sheath used to introduce an atrial and a ventricular lead; leads positioned with excellent thresholds; secured with O-silk sutures over sleeves; pulse generator connected; pocket flushed with antibiotic solution; pacemaker/leads placed in pocket; incision closed in two layers; performed under fluoroscopic guidance.
Complication:None.
Plan:Return to recovery; discharge later this evening to nursing home with routine post-pacemaker care.
Question:What CPT® coding is reported for this procedure?)
(A patient visits her provider’s office because she is experiencing persistent headaches. Her provider sends her to a radiology facility to do aCT scan of the brain without contrast. The images are sent to the provider, and the providerreads and interpretsthe scan. What CPT® coding of the radiology service is reported by the provider?)
(A patient is in her dermatologist’s office for treatment of recurring psoriatic plaques on the upper back and neck resistant to topical therapy. The dermatologist performsExcimer laser therapyon the upper back (300 sq cm) and neck (100 sq cm), total surface area400 sq cm. What CPT® codes are reported?)
(The physician performs adiagnostic ERCPof the common bile duct with insertion of astentinto the biliary duct. What CPT® coding is reported?)
A patient with intermittent asthma with exacerbation undergoes spirometry before and after bronchodilator.
What CPT® and ICD-10-CM codes are reported?
A pediatrician removes impacted cerumen using irrigation in the right ear and instrumentation in the left ear.
What CPT® coding is reported?
A woman with vulvar intraepithelial neoplasia (VIN II) undergoes a partial vulvectomy ( < 80%) with removal of skin and deep subcutaneous tissue.
What CPT® and ICD-10-CM codes are reported?
A 47-year-old male with a history of peripheral artery disease presents with worsening claudication of the left leg. A diagnostic angiography confirms stenosis in the left iliac artery. To restore blood flow to the left leg, the vascular surgeon plans to perform angioplasty, using a balloon to dilate the vessel lumen followed by placement of an expandable stent in the left iliac artery.
What CPT® coding is reported for the procedure?
A 10-year-old had a cochlear implant in his left ear few weeks ago. Today he sees the audiologist to initialize and program the implant.
What CPT® code is reported?
A 25-year-old woman underwent percutaneous breast biopsy on the right breast with placement of a Gelmark clip. The procedure was performed using stereotactic imaging.
What CPT® codes will be reported?
A 65-year-old gentleman presents for refill of medications and follow-up for his chronic conditions. The patient indicates good medicine compliance. No new symptoms or complaints.
Appropriate history and exam are obtained. Labs that were ordered from previous visit were reviewed and discussed with patient. The following are the diagnoses and treatment:
Hypokalemia - stable. Refill Potassium 20 MEQ
Hypertension - blood pressure remaining stable. Patient states home readings have been in line with goals. Refill prescription Lisinopril.
Esophageal Reflux - Patient denies any new symptoms. Stable condition. Continue taking over the counter Prevacid oral capsules, 1 every day.
Patient is instructed to follow up in 3 months. Labs will be obtained prior to visit.
What CPT® code is reported?
(A 47-year-old patient previously had a right mastoidectomy and an implanted osseointegratedBAHAdevice. Now presents with chronic infection, implant migration, and osteomyelitis of the right temporal bone. Surgeon performs arevision mastoidprocedure with debridement, removes the existing BAHA implant, and places anew osseointegrated BAHAin a new skull location. What CPT® codes are reported?)
A provider orders liquid chromatography mass spectrometry (LC-MS) definitive drug test for a patient suspected of acetaminophen (analgesic) overdose. What CPT® code is reported for the test?
A 47-year-old female presents to the operating room for a partial corpectomy on one upper thoracic vertebral body, T3. Two surgeons are performing the surgery. One surgeon performs the transthoracic approach and excises the damaged portion of the vertebral body. The second surgeon inserts a bone graft into the vertebral gap, closing the gap, and inserts a metal plate. Both surgeons work together, each as a primary surgeon.
How does each surgeon report their portion of the surgery?
A patient with three thyroid nodules is seen for an FNA biopsy. Using ultrasonic guidance, the provider inserts a 25-gauge needle into each nodule. Nodular tissue is aspirated and sent to pathology.
What CPT® coding reported?
A flexible sigmoidoscopy is performed with ablation of two sigmoid colon polyps.
What CPT® and ICD-10-CM codes are reported?
(A male patient passes out while jogging in the park. Upon examination at the hospital, he is found to have a wide complex tachycardia and undergoes anelectrophysiologic study and radiofrequency ablation. For this procedure he is placed undergeneral anesthesia. What is the anesthesia coding for this otherwise healthy 35-year-old?)
An established patient suffering from migraines without aura, no mention of intractable migraine, and no mention of status migrainosus, is seen by his ophthalmologist who conducts a visual field examination of both eyes. The examination was accomplished plotting four isopters utilizing the Goldmann perimeter testing method. The patient and requesting physician receive the interpretation and report on the same date of service.
What procedure and diagnosis codes are reported for this encounter?

TESTED 26 Jul 2026